How government policy, technology, corporate capitalization, user demand for convenience and integration will shape Massage Therapy Care
Please note, this is a draft article for Massage Therapy Canada magazine for which I’m soliciting input. What have I called correctly, in your perspective? What have I missed? Please share your perspective in the feedback space below…and thank you!
What does the future hold for the profession? While no one can know for sure, forecasting based on best available information – and a little intuition – can yield a look-see for what is trending. Forecasting can guide practitioners to fortify against risk, design their practices to remain relevant and identify new opportunities. Forecasting is essential for regulators, professional associations, training colleges and other stakeholders for resource allocation and planning for contingencies in addressing the needs of their members/students.
Here’s my speculation for the next 10+ years to come in the
massage therapy profession in Canada.
Advent of Health Technology:
The fields of bio-technology, robotics and artificial intelligence
impact all aspects of our lives. While
current massage devices appear crude, advances are being made in sensate machines
that detect pressure. Robotics are
incorporated in a variety of sophisticated applications like surgery and, linked
with artificial intelligence, will foray into the bodywork space. Mechanized
touch providing pressure and stretch to a stiff body can be applied daily and
cost-effectively and will increasingly be employed in rehabilitation and
assisted movement. This won’t replace
the personalized human touch provided by skilled practitioners but augment it. Watch for DIY (Do-It-Yourself) applications to
bodywork continue to expand.
Technology will be incorporated in patient safety, security
and quality of outcomes. Virtual Reality (VR) will expand the cognitive and
sensory experience of health care applications.
VR can enhance massage experience, but also modulate pain in the
brain. People will adopt more
sophisticated bio-sensors in all their activities, measuring heart rate, blood
pressure, and stress response. I believe
we’ll see increasingly sophisticated data generated on physiologic effects of
massage in real-time.
Personalized and Convenient
Care:
Massago provides convenient, on-demand massage services in Toronto,
Ottawa, Kitchener, Calgary and a growing list of Canadian cities. Patrons use a phone app to arrange same-day
appointments at home or alternative location, choose from a variety of massage
service types, pay for service and the rate their massage experience. Technology
verifies patron identity for the security of the practitioner. Massago aggregates user feedback to build
best practices and improve user experience over time.
While Massago addresses the on-demand market, CEO Allan Skok
shared users build a preference for an excellent practitioner and are willing
to postpone an appointment several days to get their practitioner of choice. I
expect technological improvements to lighten and strengthen portable massage
tables, make hydro/electro-therapies novel and portable to augment services.
Antithetical to the always-on, technology-saturated social
and work environments we occupy, expect the values of embodiment and mindfulness
to drive massage experience. In addition
to virtual reality integration, I expect massage practitioners to work in
tandem with practitioners of psychotherapy (who perhaps incorporate legalized psychedelic
drugs) to address deep-seated trauma, promote higher consciousness and a sense
of embodiment.
More Populations Served:
Massage therapy already serves a number of market sectors:
rehabilitation, spa/wellness, holistic/integrated care, palliative care,
athletics and work performance on-site. Adopting
a bio-psycho-social model of care, greater research literacy and capacity, and
if the profession can galvanize on government/insurer/media advocacy, we may
see massage therapists incorporated in mental health, public health, home care
and intensive rehabilitation programs.
Massage therapy may prove especially helpful in socially marginalized
populations – the poor, indigenous, victims of domestic violence, refugees, the
elderly and disabled.
Government funding and efficiencies may drive individual
disciplines to work collaboratively together – for example in home care, a
physiotherapist or nurse, massage therapist, personal support worker and social
worker. Massage therapy will continue to
be valued as an antithesis to the felt effects of aggression, violence, workplace
stress, sensory overload and trauma.
Increased Accountability Demanded by Third-Party Payers:
Insurers want accountability in claims. They want customers to use benefits
judiciously and expect health practitioners to work efficiently within financial
constraints and demonstrate efficacy in outcomes. Increasingly insurers may only fund services
that are evidence-backed. Insurers have
the ear of employers regarding cost-savings and efficiency in purchasing
employee benefit plans. We may see
massage therapy services positioned in higher cost, add-on premium insurance
products, which will reduce the number of employers signing on.
A shift to an employee spending account with a suite of options puts the user in charge of spending, hence greater scrutiny and accountability by the user for how benefit dollars are invested. Insurers may look to WSIB and auto-insurance service fee schedules and apply downward pressure on practitioner compensation for all their insurance products.
Watch for insurers to incorporate user reviews to determine preferred providers to work with, insurer control over spending and citizens actively engaged in sourcing their best health and wellness options.
Corporations and
Capitalization:
The wellness industry is valued at $4.2 trillion globally[1][2]. Massage therapy will continue to be popular, and corporations will continue to capitalize on market demand. Watch for growth in corporate employers of practitioners, high profile locations in commercial real estate hubs, strong branding and messaging, and vigorous recruiting of practitioners. Also watch for branded methods/customized protocols designed and promoted towards marketplace pain-points – similar to the many types of yoga and fitness products now available.
How do you see the future playing out? What else is trending that will affect the massage therapy field?
Please comment below or on the Facebook page.
[1] https://interestingengineering.com/3d-printed-skin-could-finally-give-robots-a-sense-of-touch
[2] https://www.globalwellnesssummit.com/2018-global-wellness-trends/
00000000
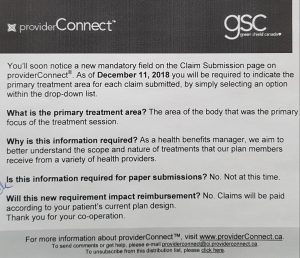 Another area to watch related to GSC, the concept of sectional therapy. GSC announced they will now be collecting data on the primary treatment area. This may be the harbinger to future claims approval linked to treating only the symptomatic areas of the body, rather than considering global bio-mechanical dysfunctions or the body-mind / psycho-social connection for the whole person.
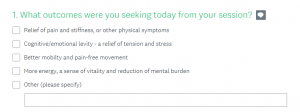
Another area to watch related to GSC, the concept of sectional therapy. GSC announced they will now be collecting data on the primary treatment area. This may be the harbinger to future claims approval linked to treating only the symptomatic areas of the body, rather than considering global bio-mechanical dysfunctions or the body-mind / psycho-social connection for the whole person.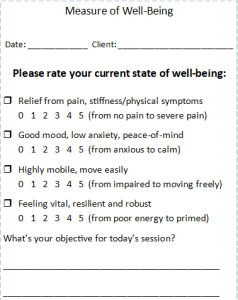 Imagine: What if an MT could measure – with every session – the impact of her/his care on 4 variables: pain relief, mood, mobility and vitality? What if collecting this data could guide an MT as to the efficacy of their care in affecting particular conditions and populations?
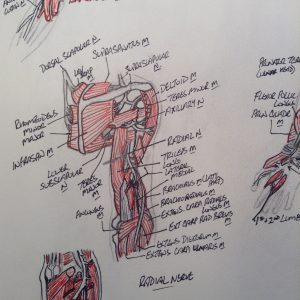
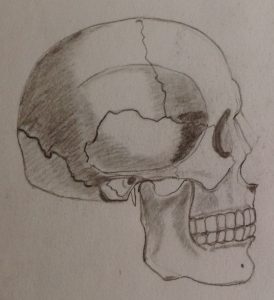
Imagine: What if an MT could measure – with every session – the impact of her/his care on 4 variables: pain relief, mood, mobility and vitality? What if collecting this data could guide an MT as to the efficacy of their care in affecting particular conditions and populations? How do you learn and appreciate anatomy? Did you use the Anatomy Colouring Book, or doodle, or find some other way to get it to stick in your memory? Can we use illustration to provide better representation of what we feel under our fingers, to give the public an in vivo look into the engagement of hands-to-body?
How do you learn and appreciate anatomy? Did you use the Anatomy Colouring Book, or doodle, or find some other way to get it to stick in your memory? Can we use illustration to provide better representation of what we feel under our fingers, to give the public an in vivo look into the engagement of hands-to-body? Calling all amateur anatomical illustrationalists out there…share your artwork!
Calling all amateur anatomical illustrationalists out there…share your artwork!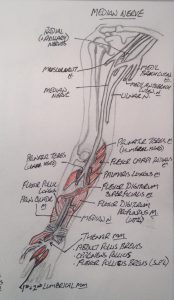







 Are you using your case history as a tool to reduce risk of harm? Would you like to build more competence in this skill? Have a look at the
Are you using your case history as a tool to reduce risk of harm? Would you like to build more competence in this skill? Have a look at the